Background: Randomised-controlled trials (RCTs) are particularly scarce and underpowered in the setting of rare diseases. The population available to study on Anderson-Fabry disease (AFD) is limited and in some studies long-term follow-up is not available.
Objectives: We present the results of a linear regression and a pooled analysis of proportions from cohort studies to evaluate the efficacy and safety of enzyme replacement therapy (ERT) for AFD in order to complement available information from meta-analysis of RCTs.
Methods: A literature search was performed, from inception to March 2016, using Medline, EMBASE and LILACS. Inclusion criteria were cohort studies, patients with AFD on ERT or natural history, and at least one patient-important outcome reported. The pooled proportion and the confidence interval (CI) are shown for each outcome. Simple linear regressions for composite endpoints were performed.
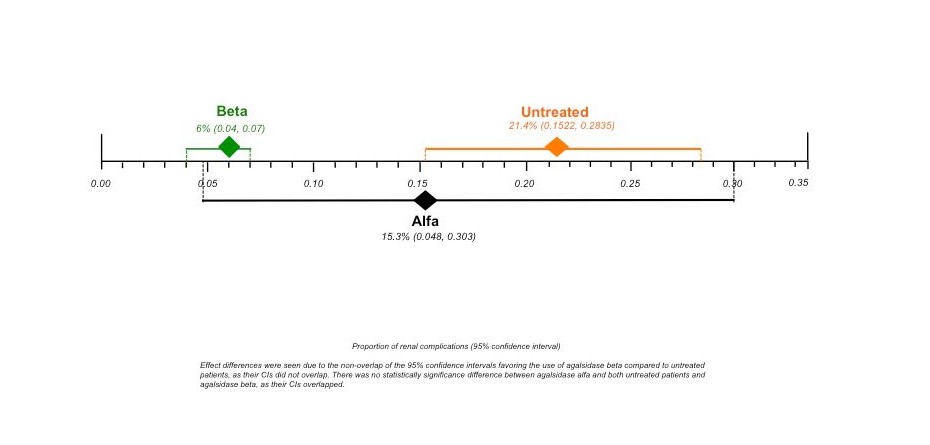
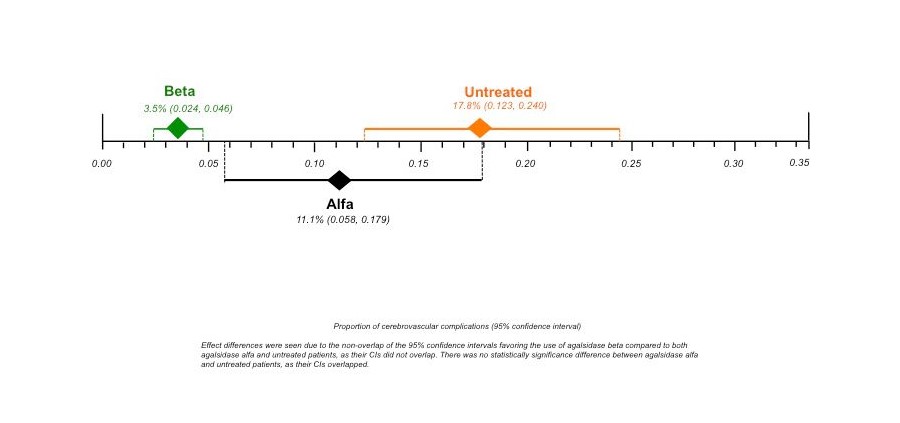
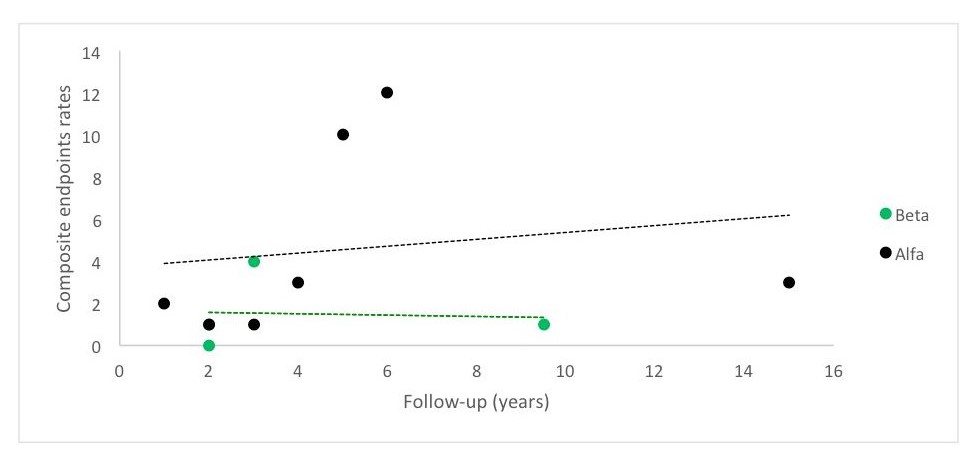
Results: 77 cohort studies involving 15 305 participants proved eligible. The pooled proportions were as follows: for renal complications, agalsidase alfa 15.3% [95% CI 0.048, 0.303; I2=77.2%, p=0.0005]; agalsidase beta 6% [95% CI 0.04, 0.07; I2 = not applicable]; and untreated patients 21.4% [95% CI 0.1522, 0.2835; I2=89.6%, p<0.0001]. Effect differences favoured agalsidase beta compared to untreated patients; and for cerebrovascular complications, agalsidase alfa 11.1% [95% CI 0.058, 0.179; I2 = 70.5%, p=0.0024]; agalsidase beta 3.5% [95% CI 0.024, 0.046; I2 = 0%, p = 0.4209]; and untreated patients 18.3% [95% CI 0.129, 0.245; I2 = 95% p < 0.0001]. Effect differences favoured agalsidase beta over agalsidase alfa or untreated patients. A linear regression showed that Fabry patients receiving agalsidase alfa are more likely to have higher rates of composite endpoints compared to those receiving agalsidase beta.
Conclusions: For rare diseases, further acquisition of knowledge needs to rely on observational studies. Accordingly due to this complementary analysis we concluded that agalsidase beta is associated to a significantly lower incidence of complications than no ERT, and agalsidase alfa.
{kind=link}
{kind=link}
{kind=link}