Background: Observational studies almost always suffer from bias because prognostic factors are unequally distributed between patients exposed or not to an intervention. The standard approach to deal with this problem is adjusted or stratified analysis. Its principle is to use measurement of risk factors to create prognostically homogeneous groups, and to combine effect estimates across groups.
Objectives & Method: The purpose of this Users’ Guide is to introduce clinicians and evidence users to fundamental concepts underlying adjustment as a way of dealing with prognostic imbalance, and the basic principles and relative trustworthiness of various adjustment strategies.
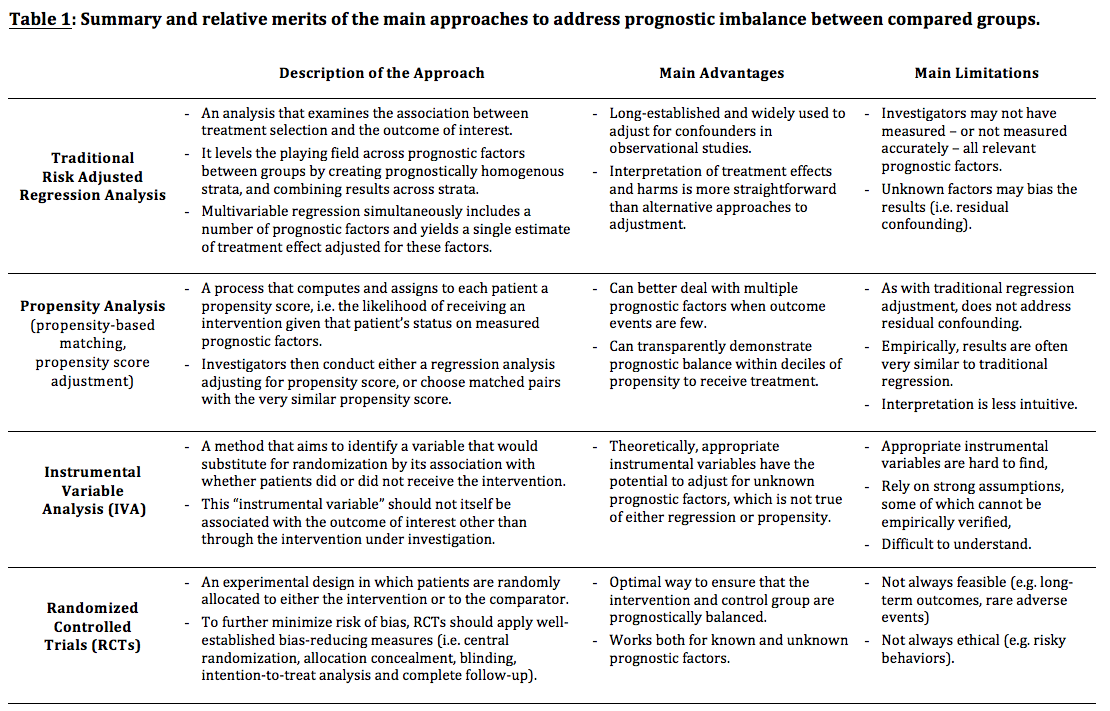
Results: Table 1 summarises the main approaches to address prognostic imbalance and their relative merits compared to randomised trials. One alternative to the standard approach is propensity analysis in which groups are matched according to the likelihood of membership in exposed or unexposed groups. Propensity methods can deal with multiple prognostic factors even if there are relatively few patients having outcome events. However, propensity methods do not address other limitations of traditional adjustment: investigators may not have measured all relevant prognostic factors (or not accurately) and unknown factors may bias the results.
A second approach, instrumental variable analysis, relies on identifying a variable associated with the likelihood of receiving the intervention but that is not associated with any prognostic factor or with the outcome itself (other than through the intervention); this could mimic randomisation. Instruments can include regional variations in healthcare, or hospitals' or physicians' practice patterns. Unfortunately, as with assumptions of other adjustment approaches, it is never certain if an instrumental variable analysis ever meets these requirements.
Conclusions: Although all these approaches can reduce the risk of bias in observational studies, none replace the balance of both known and unknown prognostic factors offered by randomisation.
{kind=link}